|
|
FAQ
1. What is endothelial dysfunction?
Endothelial dysfunction can be defined as reduced bio-availability of Nitric Oxide (NO) which plays many roles in maintaining vascular health, most importantly its role in vasomotion. Hence, endothelial dysfunction is defined as an impairment of endothelium dependent vasodilation. In their 2005 Circulation publication, Lerman et al. (1) defined endothelial dysfunction as “ultimate risk of the risk factors” a summation of the integrated affects of cardiovascular risk factor.
(1) Lerman A and Zeiher A. Endothelial Function, Cardiac events, Circulation 2005, 111,363-368.
2. What is the endothelium?
The endothelium is the inner lining of blood vessels, allowing blood to flow smoothly within them and actively maintains physiological condition. Normal endothelial function protects blood vessels from formation of atherosclerosis, the cause of cardiovascular disease.
The pathological state known as endothelial dysfunction is the earliest clinically detectable stage of cardiovascular disease (which includes heart attacks, stroke, Peripheral Arterial Disease and many other diseases). The functioning of the endothelial cells – endothelial function – is normally kept in balance. Atherosclerosis risk factors such as high cholesterol, high blood sugar, high blood pressure, smoking, aging, obesity, chronic infection, and inflammation, can all disrupt this balance and lead to endothelial dysfunction.
3. What are the consequences of endothelial dysfunction?
The main consequence of endothelial dysfunction is the initiation of an inflammatory process which leads to the formation of atherosclerosis and its late sequel, cardiovascular morbidity and mortality. Endothelial dysfunction is involved in numerous systemic disease processes such as: erectile dysfunction, metabolic syndrome, cerebrovascular diseases (stroke/TIA), pre-eclampsia toxemia, renal failure, sleep apnea, claudication, and gangrene.
4. What is the PAT signal?
The PAT (Peripheral Arterial Tone) signal is a proprietary technology used for non-invasively measuring arterial tone changes in peripheral arterial beds. The PAT signal used in the EndoPAT is measured from the fingertip by recording finger arterial pulsatile volume changes. Results of the 15-minute test are automatically calculated and an EndoScore is generated, which indicates the present state of endothelial health.
EndoPAT is the only FDA-cleared device indicated for assessment of Endothelial Function. Clearance was obtained by demonstrating equivalence of PAT Technology with an invasive catheterization procedure that directly assessed endothelial dysfunction in coronary arteries. The clinical research was conducted at the Mayo Clinic.
5. What is the EndoPAT?
The EndoPAT is the leading medical device for noninvasive endothelial function assessment. It was developed and is distributed by Itamar Medical, Caesarea, Israel.
6. How is endothelial dysfunction treated?
Endothelial dysfunction can be treated and reversed by many existing therapies such as lifestyle modification, homeopathic remedies (such as L-Arginine), drugs (e.g. statins to lower high cholesterol, ACE inhibitors used to treat high blood pressure, PDE5 inhibitor used to treat erectile dysfunction) and treatment of co-morbidities (e.g. glycemic control for diabetics). New agents that treat endothelial dysfunction specifically are under development. Endothelial dysfunction is treatable and even reversible.
7. How does the EndoPAT™ measure endothelial function?
EndoPAT™ quantifies the endothelium-mediated changes in vascular tone, elicited by a 5-minute occlusion of the brachial artery (using a standard blood pressure cuff). When the cuff is released, the surge of blood flow causes an endothelium-dependent. Flow Mediated Dilatation (FMD). The dilatation, manifested as Reactive Hyperemia, is captured by EndoPAT™ as an increase in the PAT Signal amplitude. A post-occlusion to pre-occlusion ratio is calculated by the EndoPAT™ software, providing the EndoPAT™ index.
8. Why should I get tested with the EndoPAT?
Prevention is the best treatment! Cardiovascular disease develops over many years. Initially it is a silent process, often called subclinical atherosclerosis. Endothelial dysfunction is considered to be the hallmark of subclinical atherosclerosis and the earliest clinically detectable stage. Unlike atherosclerosis, endothelial dysfunction is reversible with proper treatment.
9. Is there a threshold for a good EndoPAT™ result?
Yes, the threshold for a good EndoPAT™ result is an RHI of 1.67 and above. The threshold of 1.67 was determined following the study of Bonetti et al(6) which was performed at the Mayo Clinic. In this study the EndoPAT™ was found to be correlated with the coronary endothelial function using the gold standard method of assessment which is injection of ACH during coronary catheterization.
(6) Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr., Kuvin JT, Lerman A. Noninvasive Identification of Patients with Early Coronary Atherosclerosis by Assessment of Digital Reactive Hyperemia. JACC 2004; 44: 2137-2141
10. What should be done with the score of 1.67 and below?
EndoPAT™ score of 1.67 and below correlates to endothelial dysfunction. Endothelial dysfunction is treatable and even reversible. Endothelial dysfunction can be treated and reversed by many existing therapies such as lifestyle modification, drugs (e.g. statins to lower high cholesterol, ACE inhibitors used to treat high blood pressure, PDE5 inhibitor used to treat erectile dysfunction) and treatment of co-morbidities (e.g. glycemic control for diabetics). New agents that treat endothelial dysfunction specifically are under development.
11. Can the test been performed on children?
We rely on the medical judgment and expertise of the physician regarding the precise patient population. Although most of the testing on EndoPAT has been done on adults, there are many ongoing and published studies with the EndoPAT on children and adolescents. There is no special design of the biosensors for children, however. The length of the EndoPAT biosensor is 5cm, thus the length of the finger of the child must be at least as the length of the biosensor.
Selamet et al* tested prospectively the reproducibility and feasibility of the EndoPAT in adolescents. EndoPAT tests were performed on two different days separated by no more than seven days in 30 healthy fasting adolescents, ages 13 to 19 years. The authors concluded, “In healthy adolescents, Endo-PAT is feasible and has excellent reproducibility.” Moreover, the authors stated, “This technology may provide an easy and reliable means of assessing endothelial function in the pediatric population.”
* Selamet Tierney ES, Newburger JW, Gauvreau K, Geva J, Coogan E, Colan SD, Ferranti SD. Endothelial Pulse Amplitude Testing: Feasibility and Reproducibility in Adolescents. J Pediatr. 2009; 154(6):901-5.
12. Can the EndoPAT help predict endothelial dysfunction and cardiovascular events?
Results of a 2009 study conducted by researchers at the Mayo Clinic and Tufts reported that the EndoPAT test is “highly predictive” of a major cardiac event, such as a heart attack or stroke, for people who are considered at low or moderate risk based on their Framingham Risk Score (FRS).
The FRS is the commonly used risk predictor and was developed from the Framingham Heart Study, an ongoing longitudinal study of heart disease.
In this Mayo Clinic study, published in the Journal of the American College of Cardiology, Amir Lerman, M.D., a cardiologist at Mayo Clinic and senior author of the study, and other researchers, used an EndoPAT to measure the endothelial health of 270 patients between the ages of 42 and 66 and followed their progress between 1999 and 2007.
These patients already knew that they had low-to-medium risk of experiencing a major adverse cardiac event, or MACE, based on their FRS. Some of their risk factors included high blood pressure, high cholesterol, obesity, and a family history of heart disease.
The study results: The rate of MACE in patients who tested positive for endothelial dysfunction was 39% vs. normal endothelial function 25% (p=0.024). The study showed that patients at low FRS risk but with endothelial dysfunction were at a higher actual risk of future CV events than patients with high FRS but normal endothelial function.
Furthermore, endothelial dysfunction was found to be an independent risk factor for future MACE on multivariate analysis (p=0.002).
* Rubinshtein R, Kuvin JT, Soffler M, Lennon RJ, Nelson RE, Pumper GM, Lerman LO, Lerman A. Assessment of Endothelial Function by Peripheral Arterial Tonometry Predicts Cardiovascular Events Beyond the Framingham Risk Score. JACC 2009; Suppl.
13. How can EndoPAT, which measures changes in vascular function in a fingertip, ensure that the endothelium of the entire vascular system has been checked?
The endothelium is the same throughout the body, and when damage is noted in the fingertip, it indicates that the endothelium is damaged throughout the body—that it’s a systemic dysfunction. Endothelial dysfunction is involved in numerous systemic disease processes, including: erectile dysfunction, metabolic syndrome, renal failure, sleep apnea, and stroke.
In a study performed by Bonetti et al* at the Mayo Clinic, a group of 94 subjects underwent angiographic assessment of coronary endothelial function and subsequent EndoPAT tests. Coronary endothelial function is quantified by injection of acetylcholine during angiography.
The EndoPAT, which is a non-invasive test, was found to be highly correlative to the angiography results; it was this study that helped EndoPAT receive final FDA clearance for the detection of coronary endothelial dysfunction.
An EndoScore of 1.67 provides a sensitivity of 82% and a specificity of 77% and AUC 0.82 for diagnosing coronary endothelial function.
(*) Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr., Kuvin JT, Lerman A. Noninvasive Identification of Patients with Early Coronary Atherosclerosis by Assessment of Digital Reactive Hyperemia. JACC 2004; 44: 2137-2141.
14. How reproducible are EndoPAT results?
The EndoPAT test is both operator and interpreter independent.
Selamet et al* tested prospectively the reproducibility and feasibility of the EndoPAT. EndoPAT tests were performed on two different days separated by no more than seven days in 30 healthy fasting adolescents, ages 13 to 19 years. The authors concluded, “In healthy adolescents, Endo-PAT is feasible and has excellent reproducibility.” Moreover, the authors stated, “This technology may provide an easy and reliable means of assessing endothelial function in the pediatric population.”
* Selamet Tierney ES, Newburger JW, Gauvreau K, Geva J, Coogan E, Colan SD, Ferranti SD. Endothelial Pulse Amplitude Testing: Feasibility and Reproducibility in Adolescents. J Pediatr. 2009; 154(6):901-5.
For more information regarding EndoPAT reproducibility please address to EndoPAT product overview page 5.
15. What is the association between the EndoPAT™ and BAUS (Brachial Artery Ultrasound)?
BAUS is a common research method for peripheral, noninvasive assessment of endothelial function. It differs from EndoPAT™ in several ways. While the BAUS assesses a single conduit vessel, EndoPAT™ measures several vascular beds, composed of small vessels and microcirculation. Furthermore, EndoPAT™ corrects for systemic changes by a simultaneous measurement from the (un-occluded) contra-lateral arm. With minimal training necessary, EndoPAT™ is practically operator independent, while BAUS requires a trained ultrasound technician and is highly user-dependent in both data acquisition and analysis. Furthermore, the response measured with EndoPAT™ has a much larger dynamic range (hundreds of %) than the miniscule changes assessed by BAUS (around 10% for a normal response).Several studies have simultaneously measured Flow-Mediated Dilatation (FMD) with EndoPAT™ and BAUS. Kuvin et al.(8) at the Tufts Medical Center, Boston, demonstrated a significant correlation between the two methods (r=0.55, p<0.0001) in a group of 89 adult patients suffering from chest pain.
Read more about the association between the methods in the Product Overview page 5.
(8) Kuvin JT, Patel AR, Sliney KA, Pandian NG, Sheffy J, Schnall RP, Karas RH, Udelson JE. Assessment of Peripheral Vascular Endothelial Function with Finger Arterial Pulse Wave Amplitude. AHJ 2003; 146: 168-74
16. Is the EndoPAT correlated to coronary endothelial function?
EndoPAT provides high degrees of sensitivity and specificity when compared to the assessment of coronary artery endothelial function. Coronary endothelial function is quantified by measuring arterial diameter change and blood flow in response to graded intra-coronary infusion of acetylcholine during angiography. In a study performed by Bonetti et al* at the Mayo Clinic, a group of 94 subjects underwent angiographic assessment of coronary endothelial function and subsequent EndoPAT tests. The results of this comparative study served as the basis for the FDA clearance of the EndoPAT in the detection of coronary endothelial dysfunction. An EndoPAT index cutoff value of 1.67 provides a sensitivity of 82% and a specificity of 77% and AUC 0.82 to diagnosing coronary endothelial function.
*Bonetti PO, Pumper GM, Higano ST, Holmes DR Jr., Kuvin JT, Lerman A. Noninvasive Identification of Patients with Early Coronary Atherosclerosis by Assessment of Digital Reactive Hyperemia. JACC 2004; 44: 2137-2141.
17. What is the association between the EndoPAT and NO bioavailability?
Nohria and Gerhard et al* at the Brigham & Women’s Hospital, Boston, demonstrated the central role for nitric oxide (NO) in the post-occlusion vasodilatory response measured by EndoPAT. EndoPAT index (EndoScore) was measured in a group of nineteen healthy volunteers, before and after intra-arterial infusion of L-NAME (a specific inhibitor of endothelial nitric oxide synthase). Fifteen matched controls were infused with saline or phenylephrine (an endothelium independent vasoconstrictor). The study reported that L-NAME blocked 46% of the vasodilatory response (p=0.002). These results provide direct confirmation that EndoPAT indeed measures a NO-mediated endothelial response.
*Nohria A, Gerhard-Herman M, Creager MA, Hurley S, MitraD, Ganz P. The Role of Nitric Oxide in the Regulation of Digital Pulse Volume Amplitude in Humans. J Appl Physiol 2006; 101:545-8.
18. How well does the EndoPAT correlate with conventional cardiovascular risk factors (Framingham Risk Score)?
Since 2003, the Framingham Heart Study has included endothelial function measurements with EndoPAT. All three study cohorts (the original study population, the offspring, and the third generation cohort) have been tested with EndoPAT, totaling over 5,000 subjects.
Hamburg et al published A cross sectional analysis of 1,957 third generation subjects in 2008*. The study demonstrated a significant inverse relation between EndoPAT index and multiple CV risk factors, including: male sex, body mass index, total/HDL cholesterol, diabetes, smoking, and lipid-lowering treatment.
*Hamburg NM, Keyes MJ, Larson MG, Vasa RS, Schnabel R, Pride MM, Mitchell GF, Sheaf J, Vita JA, Benjamin EJ Cross-Sectional Relations of Digital Vascular Function to Cardiovascular Risk Factors in the Framingham Heart Study. Circulation 2008; 117: 2467-2474.
19. How long does the EndoPAT™ test take to complete?
The test takes 15 minutes to complete, is very easy to perform, and is both operator and interpreter independent. It is a noninvasive test, providing automatic analysis, office-based procedure.
20. Why does the EndoPAT test require using both arms?
Think of the EndoPAT evaluation as a one-person clinical study with you comparing yourself to yourself. While endothelial function is being tested in one arm with the blood pressure cuff and finger monitor, your other arm is being used to monitor changes in blood flow that generally affects both arms. By then measuring both arms, EndoPAT automatically corrects for any systemic changes that may occur during the course of the test and calculates a final EndoScore based on information gathered from both finger monitors.
21. Which arm should be used for occlusion/control?
The non-dominant arm is recommended as the tested (occluded) arm due to a lower mass of muscle and leads to easier arterial occlusion.
22. Does it matter which fingers are used for the test?
Any finger but the thumb may be used. But placement of the sensors on the index fingers is recommended. Due to variance between fingers in blood supply symmetrically-paired fingers on both arms should be used (i.e. either both index fingers or both middle fingers). The thumb should be avoided.
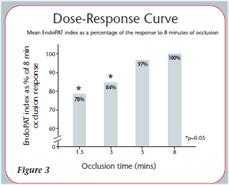
23. Why does the occlusion last 5 minutes?
Five minutes is the optimal time needed to generate the forced stimulus response of the blood rushing through the vessels in response to an occlusion. Faizi et al. (4) tested the effects of varying occlusion durations as well as the effects of occlusion location in 30 apparently healthy adult volunteers. When comparing different occlusion times (1.5, 3, 5 and 8 minutes) with the cuff placed on the forearm, they saw that the effective maximal response was reached at 5 minutes. The occlusions shorter than 5 minutes had significantly lower responses. The response to a 5 minute occlusion did not differ significantly from 8 minutes, but caused less discomfort.
24. Does having the blood pressure cuff inflated on the upper arm for five minutes cause any discomfort?
The five-minute blood pressure cuff inflation is an accepted standard test to cause reactive hyperemia (the increase of blood flow after a temporary restriction in blood supply) for the assessment of endothelial function. While the occlusion may cause some minor discomfort and tingling in the fingers, the test is absolutely harmless.
25. Where should we place the blood pressure cuff for the occlusion?
Optimal location is on the upper arm. Faizi et al. (5) tested twenty individuals with the cuff placed on their upper arm, occluding the brachial artery for 5 minutes. These results were compared to their 5 minute forearm occlusion test, showing an EndoPAT™ index of 1.88 (±0.55) for the forearm occlusion and 2.07 (±0.69) for the upper-arm occlusion (p=0.097). Forearm occlusion was reported to cause less discomfort than the upper arm.
(5) Faizi AK, Kornmo DW, Agewall S. Evaluation of Endothelial Function Using Finger Plethysmography. Clin Physiol FunctImaging 2009 Jun 22.
26. What are the clinical setting requirements for the EndoPAT™ test?
The EndoPAT™ is compact and can be used in almost any clinical setting. Since the PAT signal reflects autonomic nervous system activity, it is recommended to create a stress free environment during the EndoPAT™ test. The room selected for the study should be in a quiet area, thermo-neutral room temperature should be maintain 21oC-24oC (70oF-75oF) and dimmed lights are preferred when performing the study. The test can be performed on a comfortable bed, exam table or armchair which will enable placing both hands at heart level in a rested position.
27. Is there any special patient preparation needed before an EndoPAT test?
It’s recommended that the patient fast 3 to 8 hours before the test. In addition, the following drugs should not be used for 24 hours before testing:
 | Nitroglycerine |
| Alpha-blockers, beta-blockers, and calcium channel blockers |
| ACE inhibitors |
| Statins |
28. What is the RHI and how it is calculated?
RHI stands for Reactive Hyperemia Index. This is the final concluded result of the EndoPAT™ test. It is a ratio of the post-to-pre occlusion PAT amplitude of the tested arm, divided by the post –to-pre occlusion ratio of the control arm.
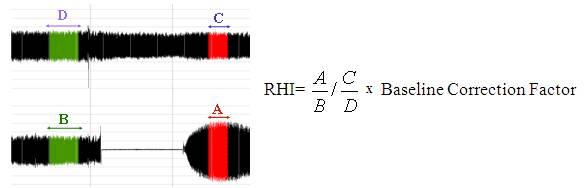
A - Mean PAT amplitude between 90s-150s post occlusion of the occluded arm
B - Mean PAT amplitude from the baseline period of the occluded arm
C - Mean PAT amplitude between 90s-150s post occlusion of the control arm
D - Mean PAT amplitude from the baseline period of the control arm
29. How do I get a result from the device and in what formats?
The output of the EndoPAT™ is presented as follows:
| A printable report with the test result, parameters and a graph of the test, which can be attached to the patient’s chart. |
| A spreadsheet with multiple test variables and quality control parameters for in-depth assessment. |
30. How is EndoPAT data saved?
Data is saved in the EndoPAT hard drive. It is possible to transfer files and review it on another computer as long as it has the EndoPAT software installed.
31. How can I send the EndoPAT™ data to Itamar-Medical experts?
If the physician has any question regarding a specific EndoPAT™ test that he whish to consult with Itamar-Medical experts, he may send the row data to Itamar-Medical ftp server. Please see the instructions attached.
32. Has the U.S. Food and Drug Administration approved the EndoPATfor diagnostic use?
Yes, in 2003. The EndoPAT is the only FDA–cleared device indicated for assessment of endothelial function
33. What is an EndoPAT test?
An EndoPAT (Peripheral Arterial Tone) test is a non-invasive evaluation of the overall health of the endothelium. Normal endothelial function protects the blood vessels from atherosclerosis (hardening of the arteries) and plaque buildup. The test, which can be performed in a doctor’s office, takes 15 minutes.
34. Can endothelial dysfunction be reversed?
Yes. Improving the health of the endothelium entails eating less fat, not smoking, lowering cholesterol, exercising on a regular basis, and taking medications (e.g.; statins to lower high cholesterol, ACE inhibitors for high blood pressure, PDE5 inhibitors for erectile dysfunction) and vitamins as prescribed by your physician.
35. How does the EndoPAT test work?
The EndoPAT is a simple six-step test:
| Step One: With the patient lying comfortably on the examination table, a standard inflatable blood pressure cuff is placed around the bicep. The other arm without the cuff will serve as the control in the test. |
| Step Two: Special finger biosensors containing plethsymographic probes, which are connected to the EndoPAT recording device, are placed over the index finger of each hand to monitor the function of the blood vessels. A reading of the fingers’ blood flow rate begins and measures Peripheral Arterial Tone, or PAT, which is the special way that pulse waves travel from the heart, throughout the body, and are then reflected back again. |
| Step Three: After having PAT monitored while resting comfortably for 10 minutes, the blood pressure cuff on the left arm is inflated, which temporarily stops the flow of blood through the left arm and hand. |
| Step Four: After five minutes, the blood pressure cuff is deflated, releasing blood flow through the brachial artery to the fingers. |
| Step Five: The special finger sensors monitor reactive hyperemia, which is the normal blood flow response that occurs when the blood pressure cuff is released and blood returns to the finger tips. |
| Step Six: The EndoPAT then automatically converts the changes in PAT into a graph, which is used to assess the blood vessels and their hyperemic response before, during, and after the arm cuff was used on the brachial artery. |
36. What is an EndoScore?
An EndoScore is the final analysis of a 15-minute EndoPAT assessment based on the ratio of the post- to pre-occlusion PAT amplitude of the tested arm, divided by the post- to pre-occlusion ratio of the control arm.
The higher the EndoScore, the better the health of the endothelium and the lower the risk for heart disease.
There are three basic categories for EndoScores:
| Red Zone: Score of 1.68 and lower. You do not have proper endothelial function and this could be an important signal of an imminent cardiac problem. This EndoScore may indicate the presence of disease and that an immediate evaluation and intervention may be needed, whether it is aggressive medical therapy or a medical procedure. It’s imperative that endothelial health be restored. |
| Yellow Zone: Score between 1.69 and 2. Your endothelium is healthy and while you don’t have any additional risk, you are still not in the well-protected Green Zone. It’s vitally important that you now take charge of your own health and do everything you can to improve your EndoScore. Good health depends of certain lifestyle choice you make that include what you eat, how active you are, whether or not you smoke, the precautions you take to avoid injuries and accidents, and how you deal with tension and anxiety. The choice is yours. Choose health! |
| Green Zone. Score between 2.1 and 3. Your endothelium is functioning optimally, and you have maximum protection. Keep up whatever it is that you are doing, because the foods that you have been eating and the physical activity you have been performing regularly have affected a number of risk factors implicated in vascular health and longevity, particularly blood cholesterol levels, hypertension, and obesity. |
37. Who should have an EndoPAT test?
The earlier you diagnose a cardiac condition and initiate a cardio-protective program, the better off you are. Candidates include men between the ages of 40 and 70 and women between the ages of 50 to 70 with one or more of the following risk factors for heart disease:
| Diabetes |
| Cigarette smoking |
| Elevated cholesterol level |
| Family history of heart disease (sudden death, heart attack, or need for angioplasty or bypass surgery) in a first-degree male relative (parents or siblings) 55 years old or less, or a first-degree female relative 65 years old or less. |
| High blood pressure |
| Obesity |
| Sedentary life style |
If you have multiple risk factors, or one particularly severe risk factor, you need to talk to your physician about earlier intervention. For example, if you are a 35-year-old male and your father died at the age of 41 of a heart attack, an EndoPAT test would be warranted.
38. What information does the EndoPAT provide?
From the information gathered during an EndoPAT test, the following can be assessed:
| Early detection of atherosclerosis (hardening of the arteries) |
| Blood circulation status |
| Disturbances in the smaller blood vessels not found when measuring blood pressure with a standard blood pressure cuff. |
39. Should I have the EndoPAT test performed if I don’t have any risk factors for heart disease?
Absolutely. Many patients are having the EndoPAT test performed strictly for preventive reasons as a way to quantify their ongoing health maintenance strategies. Even though there are quite a few who end up with very high Yellow Level and Green Level EndoScores, EndoPAT testing has also uncovered underlying coronary artery disease in many asymptomatic patients.
40. What are endothelial cells?
These are the cells that comprise the endothelium, the interior surface of the entire 60,000-mile circulatory system, including the heart and all the blood vessels of the body. Endothelial cells make and release nitric oxide, a simple molecule that causes blood vessels to relax and open, allowing for maximum blood flow. Endothelial cells also make endothelin, a substance that causes blood vessels to constrict. It’s these two important molecules that enable blood vessels to widen and narrow instantaneously in response to the oxygen demands of nearby tissues.
41. Why are endothelial cells important?
In addition to ensuring maximum blood flow to the tissues, endothelial cells help protect blood vessels from atherosclerosis, a hardening of the arteries that is caused by buildup of plaque in the arteries.
42. What causes endothelial damage and endothelial dysfunction?
The endothelium can be damaged by cigarette smoke, high cholesterol, elevated blood and insulin levels, high blood pressure, nutrition deficiencies, lack of exercise, and chronic stress.
43. How does endothelial dysfunction affect cardiovascular health?
When smoking, fatty foods, and pollutants damage the endothelium, this leads to chronic inflammation, damage to endothelial cells, and dysfunctional blood vessels. Over time, this can cause the blood vessels to stiffen, leading to high blood pressure, heart attack, stroke, peripheral artery disease, erectile dysfunction, metabolic syndrome, sleep apnea, renal failure, and gangrene.
44. Why should the health of the endothelium be tested?
Prevention is the best treatment! It’s important to regularly gauge the well-being of the endothelium system because the overall health of the heart and circulatory system depends on the optimal functioning of this thin layer of cells that line insides of all the blood vessels and the heart. Cardiovascular disease develops over many years, initially as a silent process. Damage to the cells that comprise the endothelium is the earliest clinically detectable stage of cardiovascular disease.
45. Is the EndoPAT test used in cardiac-related research studies?
The EndoPAT has been used in dozens of clinical studies conducted at such renowned medical institutions as The Mayo Clinic, Johns Hopkins Medicine, Harvard Medical School, Cleveland Clinic, the Framingham Heart Study, and Mount Sinai Hospital (NY).
46. How is the EndoScore delivered?
When the EndoPAT test is completed, a report will be printed that includes test results and a detailed graph of the test. In addition, a spreadsheet with multiple test variables and quality control parameters will also be printed for in-depth assessment.
47. Do health insurance carriers cover EndoPAT testing?
In many cases, EndoPAT is an elective test that may not be covered by health insurance plans. Be sure to check with your own insurance carrier.
48. Where can I have an EndoPAT test performed?
Whether you are at high risk or just wish to have a test to establish a baseline for future comparison, contact us or check Dr. Near You for a doctor or health facility nearest you who performs the testing
|
|